Self-Care and Human Needs
Self-care is one of the hot topics these days in the world of bipolar disorder and the people who live with it. Self-care can be as basic as remembering to eat or as complicated as knowing and avoiding your triggers.
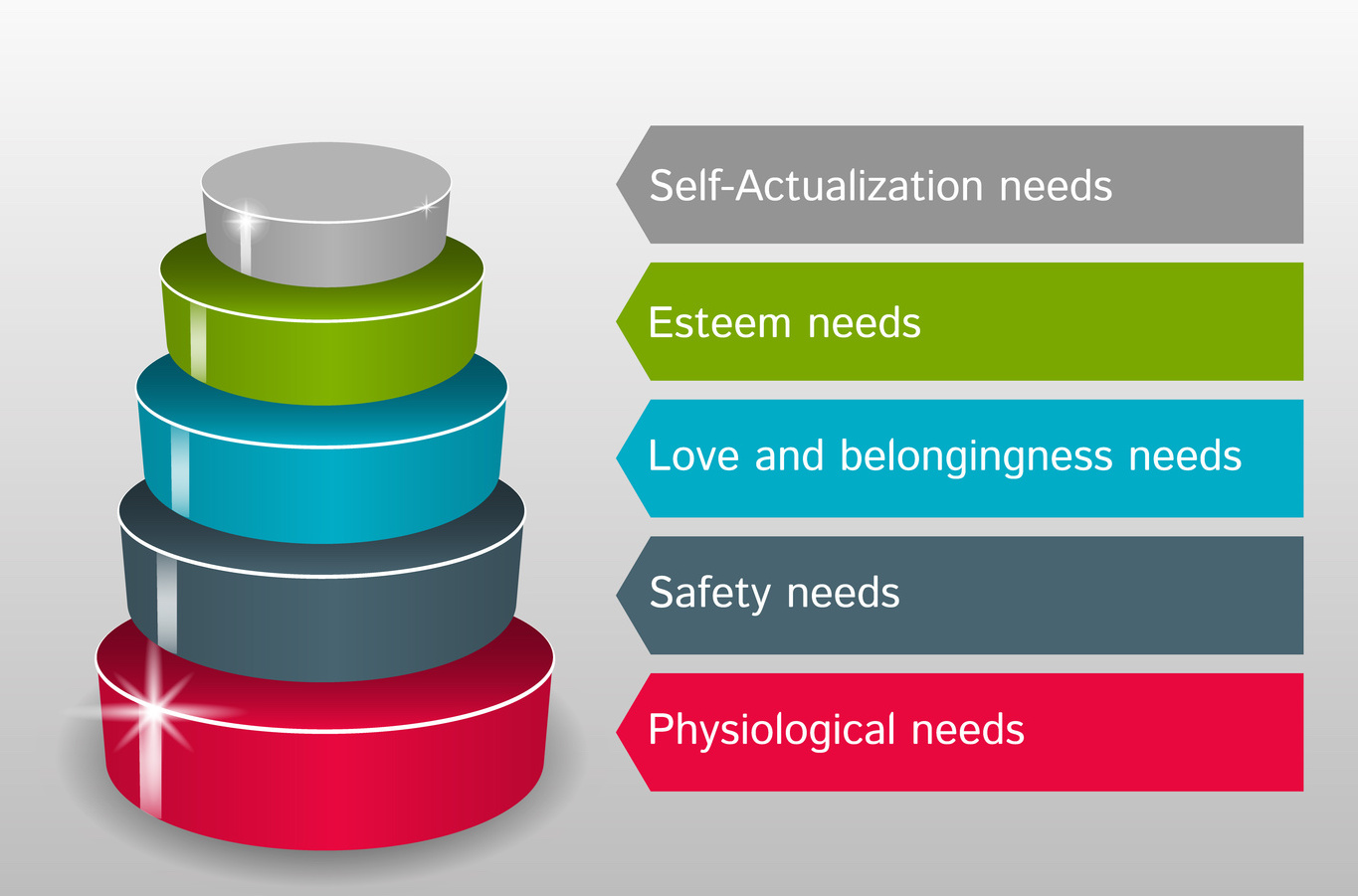
Back in 1943, psychologist Abraham Maslow created what he called a “hierarchy of needs” – a series of stages that human beings must go through on the way to the ultimate goal of “self-actualization.” With few changes, the concept, usually illustrated as a pyramid, has continued to influence the study of human motivation and developmental psychology.
So what does self-care have to do with the hierarchy of needs?
The most basic needs of human life form the base of the pyramid. These are called “physiological needs” and are essentially what a person needs to stay alive: air, water, food, shelter, sleep, clothing. Without meeting these needs, a person cannot move up to the next level of the hierarchy.
A large part of self-care is devoted to meeting these very basic, fundamental needs. Air is usually not a problem but shelter and clothing can be, for those bipolar persons who are homeless – and there are more than a few. Many of us are just one financial reverse – loss of income, insurance, options – from being homeless.
The most common advice for self-care is to pay attention to these base-level needs: Remember to eat. Stay hydrated. Get enough sleep. At times, it’s a real struggle just to meet these self-care needs. Add “get exercise” to the list and it can suddenly be overwhelming. People with bipolar or major depressive disorder often need help accomplishing them. That’s as high as we get on the pyramid.
The second step of the pyramid, which people need to work on after they’ve met the requirements of the first step is called “safety needs”: personal security, employment, resources, and health. Again, the needs on this step may seem insurmountable, and may – probably will – require help to achieve.
But they are self-care needs too. Current society may not view them as such, but that’s because they tend not to struggle with them, at least not on the level of a person with a mental disorder. Individuals can sometimes help meet these needs, but more often government, community, or charitable organizations provide necessary help. Talking about self-care at this second level may seem like pie-in-the-sky to those who have not yet conquered the first. But truly, taking care of these needs is a form of self-care, enabling one to maintain the gains represented by achieving those of the first level.
The third level of human needs – and self-care – is called “love and belonging”: friendship, intimacy, family, sense of connectedness. Again, this is not usually thought of as a part of self-care. But it certainly is. Many of us – I include myself – lose friends, become estranged from family, fail at intimate relationships. There are other places to look for ways to practice self-care on this level, however.
Therapy groups and self-help groups can lead you to people who share your problems and may be able to help you in achieving self-care. (My husband met one of his dearest friends, who provided support, listening, understanding, and companionship, at a self-help group meeting.) If in-person meetings are not possible, social media such as Facebook, Twitter, and WordPress provide opportunities to meet some social self-care needs through various groups and online communities.
The top two levels of the pyramid are not as easy to think of as self-care, and not as easy to tackle. Level four is esteem: respect, self-esteem, status, recognition, strength, freedom. And five is self-actualization: to become the most that one can be. Realistically, these are not strictly speaking things that can be accomplished through self-care. Even neurotypical people may never complete step four, and there is reason to think that few people ever reach self-actualization. These are goals to strive for, but not guarantees.
Wherever you may currently be on the pyramid, the important thing to remember is that self-care will help you reach the next step; that each follows the one before; and that your bipolar life will improve with every step you achieve.









Recent Comments